Are your hypertension claims getting denied due to vague or incorrect diagnosis codes? Uncontrolled HTN ICD-10 coding remains a persistent problem across primary care, cardiology, and internal medicine practices. In 2026, industry estimates place initial claim denial rates for chronic condition diagnosis errors between 11% and 15%, with hypertension-related coding mistakes ranking among the top triggers.
The financial stakes are real. Practices spend $25 to $117 reworking each denied claim. Nearly 60% of denied claims never get corrected or resubmitted. Billing teams that misapply hypertension diagnosis codes also face audit exposure under CMS chronic condition documentation standards.
This article covers the correct ICD-10 codes for uncontrolled hypertension, essential HTN coding rules, how to link diagnosis to medical necessity, common billing errors, and prevention strategies across your revenue cycle.
What Is the ICD-10 Code for Uncontrolled HTN?
Understanding how ICD-10 classifies hypertension is the first step toward clean claim submission. The ICD-10-CM code set does not include a standalone “uncontrolled hypertension” code. That distinction matters for every billing team submitting hypertension claims.
ICD-10 classifies hypertension by type and complication, not by control status alone.
The Primary Hypertension ICD-10 Code
The standard ICD-10 code for hypertension is:
I10 — Essential (primary) hypertension
This code covers:
- Hypertension without documented complications
- High blood pressure with no identified secondary cause
- Essential hypertension ICD-10 billing for most outpatient encounters
- Uncontrolled hypertension when the provider documents elevated readings without organ involvement
- Benign hypertension ICD-10 scenarios under prior classification systems
I10 is an unspecified hypertension ICD-10 code in the sense that it does not differentiate control status. When a provider documents “uncontrolled hypertension,” I10 remains the correct code unless a complication is documented.
When to Use Additional Hypertension Codes
Hypertension with documented organ involvement requires more specific coding. Using I10 alone when complications exist is a common coding error.
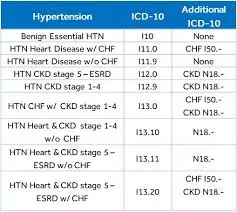
Key codes beyond I10 include:
- I11.0 — Hypertensive heart disease with heart failure
- I11.9 — Hypertensive heart disease without heart failure
- I12.9 — Hypertensive chronic kidney disease, stage 1–4
- I13.10 — Hypertensive heart and CKD without heart failure
- R03.0 — Elevated blood pressure reading, no diagnosis of hypertension
- O10.012 — Pre-existing essential hypertension in pregnancy
Do not use R03.0 when hypertension is a confirmed diagnosis. That code applies only when elevated readings exist without a formal hypertension diagnosis.
Hypertension ICD-10 Coding Guidelines: What Coders Get Wrong
The AHA/AHIMA coding guidelines and CMS documentation requirements address hypertension directly. Most billing errors stem from ignoring the distinction between presumptive coding and confirmed diagnosis coding.
“Uncontrolled” Is a Descriptor, Not a Code
ICD-10-CM does not assign a separate code for uncontrolled blood pressure ICD-10 scenarios. Providers who document “uncontrolled HTN” are describing the clinical status, not directing the coder to a different code.
Common coding errors include:
- Searching for a standalone “uncontrolled hypertension ICD-10 code” that does not exist
- Using R03.0 for patients with a known hypertension diagnosis
- Applying outdated ICD-9 logic (401.1 benign, 401.0 malignant) to ICD-10 claims
- Omitting complication codes when the record documents hypertensive heart disease
- Failing to link I10 to associated cardiovascular or renal conditions
When the provider documents “HTN, uncontrolled” with no organ complication, report I10. When complications exist, report the appropriate I11–I13 combination code.
Stage 2 Hypertension ICD-10 Coding
ICD-10-CM does not classify hypertension by ACC/AHA stages (Stage 1, Stage 2). The staging system used in clinical practice does not map to separate ICD-10 codes.
Stage 2 hypertension ICD-10 billing still uses I10 unless:
- Heart disease is documented (use I11.x)
- Chronic kidney disease is documented (use I12.x)
- Both are present (use I13.x)
Coders who attempt to find a stage-specific code create specificity errors that trigger CO-16 denials for insufficient documentation.
Hypertension Diagnosis Code Errors That Trigger Denials
Most hypertension billing denials fall into three categories: wrong code selection, missing linkage to complications, and documentation gaps. Practices that audit ICD-10 hypertension codes quarterly find and correct these errors before they compound.
Diagnosis Linkage Failures
Payers apply medical necessity edits that require proper diagnosis linkage between the hypertension code and any associated procedure or E/M service.
Denial triggers related to linkage include:
- Billing an E/M visit without documenting how HTN management justifies the level of service
- Submitting cardiac monitoring CPT codes without linking I10 or I11.x as the primary diagnosis
- Using R03.0 alongside antihypertensive prescriptions, which contradicts coding guidelines
- Failing to report secondary codes for CKD when both conditions are managed at the same visit
- Omitting hypertension from the problem list despite active medication management
Chronic Hypertension ICD-10 Documentation Gaps
Chronic hypertension ICD-10 coding requires consistent provider documentation across encounters. Payers audit for documentation that supports ongoing condition management.
Specific documentation failures include:
- No blood pressure reading documented in the visit note
- Provider writes “HTN controlled” but no code or problem list update appears in the chart
- Visit focused on another complaint with hypertension listed only in the past medical history
- Prescription refill encounters coded without supporting visit documentation
- No mention of medication response or dosage adjustment for uncontrolled readings
Step-by-Step Workflow for Correct Hypertension ICD-10 Billing
A structured coding and billing workflow reduces hypertension diagnosis code errors before claims reach the payer. Practices using this approach report measurable improvement in first-pass rates within 60 to 90 days.
Hypertension Coding Workflow
- Confirm the provider has documented a hypertension diagnosis, not just a blood pressure reading.
- Review the encounter note for any documented complications (heart disease, CKD, pregnancy).
- Select I10 for essential hypertension with no documented complications.
- Add I11.x, I12.x, or I13.x when organ complications are documented in the same note.
- Remove R03.0 from any claim where a confirmed hypertension diagnosis exists.
- Link the hypertension ICD-10 code to any associated procedure or monitoring service billed on the same date.
- Verify the diagnosis code supports medical necessity for any ordered lab work, ECG, or imaging.
- Run the claim through payer-specific diagnosis edits before submission.
- Review ERA responses within 48 hours and flag any CO-16 or CO-50 denials for same-day correction.
When to Appeal vs. When to Resubmit
Resubmit claims when:
- Wrong ICD-10 code was entered due to a data entry error
- R03.0 was used instead of I10 despite confirmed diagnosis in the chart
- Complication code was omitted but the documentation clearly supports it
File an appeal when:
- Payer denies medical necessity despite documented uncontrolled readings
- CO-50 denial was applied to an established hypertension management visit
- Payer incorrectly bundles hypertension management into a preventive visit
Key point: Technical coding errors go to resubmission. Payer policy disagreements go to formal appeal with clinical documentation attached.
Prevention Strategies for Hypertension Billing Code Errors
Preventing diagnosis coding errors requires attention at every stage of the revenue cycle. Front-end intake, provider documentation, and back-end audit processes all affect hypertension claim accuracy.
Front-End Prevention
Patient access and intake teams set the foundation for accurate hypertension billing.
Key front-end controls:
- Confirm the active problem list includes the correct hypertension diagnosis before each visit
- Flag charts where R03.0 is listed alongside active antihypertensive medications for coder review
- Verify payer coverage for hypertension management visits, especially Medicare Advantage plans
Mid-Cycle Prevention
Coding and documentation accuracy during charge entry prevents the most expensive denials.
Common mid-cycle errors to correct:
- Applying stage-based codes that do not exist in ICD-10-CM
- Selecting I10 without reviewing the note for undocumented cardiac or renal complications
- Failing to update the claim when the provider amends the note post-visit
Back-End Prevention
Billing follow-up teams catch errors that passed through front-end and coding review.
Key back-end controls:
- Track hypertension ICD-10 denial patterns by payer and denial code monthly
- Flag CO-16 denials on hypertension claims for documentation review within 5 business days
- Audit primary vs. secondary diagnosis sequencing on multi-condition encounter claims quarterly
Conclusion
Hypertension coding errors persist because providers, coders, and billing staff apply different assumptions to the same documentation. The absence of a standalone “uncontrolled hypertension ICD-10 code” creates consistent confusion, and that confusion converts directly into denied claims and delayed reimbursement.
The solution is straightforward: use I10 as the default essential hypertension ICD-10 code, add complication-specific codes when documentation supports them, and never substitute R03.0 for a confirmed hypertension diagnosis. Apply that logic consistently at every stage of the revenue cycle.
Practices that implement these coding controls and conduct quarterly ICD-10 hypertension audits reduce denial rates, improve first-pass claim performance, and reduce the administrative cost of rework across primary care and cardiology billing workflows.
FAQs
What is the correct ICD-10 code for uncontrolled hypertension?
ICD-10-CM does not have a separate code for uncontrolled hypertension. When a provider documents uncontrolled HTN without organ complications, report I10 (Essential hypertension). If cardiac or renal complications are documented, add the appropriate I11, I12, or I13 code.
What is the difference between I10 and R03.0 for hypertension billing?
I10 applies when a provider has formally diagnosed hypertension and it appears on the active problem list or in the assessment. R03.0 applies only when a blood pressure reading is elevated but no hypertension diagnosis has been established. Using R03.0 for a patient with a known hypertension diagnosis violates ICD-10-CM official coding guidelines.
Does ICD-10 have a code for Stage 2 hypertension?
No. ICD-10-CM does not use ACC/AHA staging terminology for hypertension codes. Stage 2 hypertension still maps to I10 unless heart disease or CKD is documented, which would require I11.x or I12.x respectively. Coders who search for a stage-specific code often create unspecified or incorrect code submissions.
Which ICD-10 codes apply when hypertension and chronic kidney disease are both present?
Use the I13.x combination codes when both hypertensive heart disease and CKD are documented. For CKD alone with hypertension, report I12.9 (or I12.9 with the CKD stage code N18.x appended). Do not report I10 and N18.x together when a hypertensive CKD combination code is available.
What denial codes appear most often on hypertension ICD-10 billing errors?
CO-16 (missing or incomplete information) appears when diagnosis documentation does not support the code submitted. CO-50 (non-covered service) appears when medical necessity fails payer edits. CO-97 appears when the hypertension diagnosis is bundled incorrectly with another covered service. Billing teams that categorize hypertension denials by CO-code resolve patterns faster and prevent repeat submissions.